
Visit 1
36 y.o. male with no pmhx presents with 4 days prior pt had chills and fatigue with fever up to 103.5. Today became nauseated lightheaded and had a syncopal episode. Did not hit head. Also complaining of a pruritic red rash to his bilateral lower extremities that spread to diffusely his arms, palms, neck, and face this morning. Recently seen by pcp who thought symptoms 2/2 virus and scheduled to see a dermatologist tomorrow.

Vitals: Temp: 103 °F (39.4 °C) BP: (unable) Pulse: 118 Resp: 16 SpO2: 91 %
Physical Exam - Pertinent positives
Erythematous patchy rash with occasional small bola on all 4 extremities and extending to palms of hands bilaterally.
Now what?
Ddx for rash/fever/lightheadedness?
Labs?
Imaging?
Results
CXR - Negative
WBC - 7.7
HGB - 15.9
Platelets - 143
%Neutrophil - 91.2
%Lymph - 2.9
HGB - 15.9
Platelets - 143
%Neutrophil - 91.2
%Lymph - 2.9
Chemistry - ALT 149, AST 64, Alk phos 137 all other normal
Dispo
Discharged home with symptomatic care and dermatology appointment tomorrow.
__________________________________________________________________
__________________________________________________________________
Visit 2 (the next day)
36 y.o. male with no PMHx presents with syncope and rash. Recently in wedding in Wisconsin after returning he developed a fever, chills, shakes, and a stiff neck. Rash developed two days later which greatly progressed to his whole body today (including his arms, legs, stomach, back, face, and bilateral palms) Patient had a syncopal episode yesterday after he had returned home from seeing his PCP. Came to ED began feeling better went to dermatologist today at which time he had biopsies taken but today he had another syncopal episode after he took a 3-4 hour nap.

Also complaining of "bad" headache, and is unable to urinate. No new medications, cp or sob.
First Vitals: Temp: 100.3 °F (37.9 °C) BP: 110/61 mmHg Pulse: 105 Resp: 18 SpO2: 98 %
Physical Exam - Pertient positives
Blanching erythematic macules over lower extremities. Greater concentrations by the knees. Warm to touch. Macules across the chest. Macules become confluent. Small macules over bilateral palms.

We have a bounce back?
What should we do differently?
Before we get to results…consider a "cognitive pause"
Confirmation Bias
Clinicians accentuate confirmatory data and ignore non confirmatory data
A pitfall in emergency medicine leads to inaccurate diagnosis and inappropriate treatments and care plans
Use of heuristics or protocols increase this risk
Treatment = Metacognition. A reflective approach to problem solving
This is to be used in error-producing conditions (ie low prevalence high mortality conditions)
A patient returning to the ED is among the highest risk patients for confirmation bias; do something new
Prior Results:
WBC - 11.2
Hgb - 15.3
Hgb - 15.3
Platelets - 139
Neut% 92.7
Lymph% 2.8
Chemistry - ALT 149, AST 64, Alk phos 137 all other normal
New Tests and results:
CSF - "pleocytosis" with Protein 23.9 Glucose 54
Ehrlichia - Negative
Lyme - Negative
Things aren’t looking that bad until...
Second Vitals: BP 70/42 HR 135 Resp: 22 SpO2:98%
Central Line placed, 2L completed IV pressors started
Broad spectrum antibiotics + doxycycline
What did we miss?
Fever+Rash+Syncope = shock
Now we just need to find the etiology of the shock
Tick borne illness
SJS/TEN
Mononucleosis
Viral hepatitis
Streptococcal
Primary HIV
Secondary syphilis
Parvovirus
Kawasaki
Meningitis
Myocarditis/Pericarditis
Rheumatologic (is everything still Lupus?)
Final Differential Diagnosis:
Infectious > drug rash > rheumatologic
WARNING: READ ON FOR THE ANSWER
_____________________________________________________
Tick Borne Illnesses
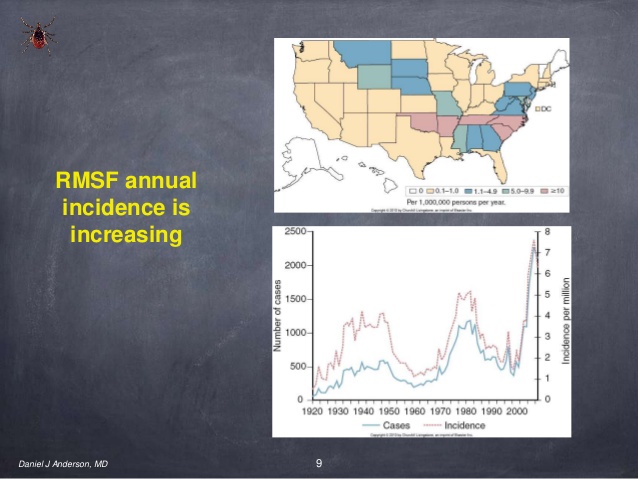
Working diagnosis: RMSF Rickettsiea Rickettsii
2000 cases/year in US, 1 death MN in 2009, Transmitted by Brown Dog Tick
Presentation
Majority of patients seek care at 2--4 days of onset of illness, early signs very nonspecific mimicking viral illness. 60-75% of patients receive an alternative diagnosis on their first visit for medical care.
Key words: Severe headache, three days later rash
90% of patients have a rash usually 2-5 days AFTER fever, initially small pink macules on wrists/ankles LATER petechia
Splenomegaly
Labs - nonspecific really just ruling out other causes
- Thrombocytopenia (may also have anemia and leukopenia)
- Mild transaminitis
- Hyponatremia (especially with central nervous system involvment)
- May progress to coagulopathy and DIC
- 19% developed ARF
- CSF analysis - elevated protein with normal glucose, only IGM indicates local production, often pleocytosis
- Skin biopsy can be used for definitive diagnosis
- Blood cultures sensitive and specific
DDx
Stevens-Johnsons, Mononucleosis, viral hepatitis, ehrlichiosis, streptococcal, Primary HIV, secondary syphilis, parvovirus, Kawasaki, Meningitis,
Treatment
Doxycycline
Mortality
Declined 2000 to 2007 from 2.2% to 0.3%
Fatality highest in age younger than 4 and greater than 60 yo
What about that Biopsy?
When do we consult Dermatology?
High risk dermatologic conditions = Acute in onset, blistering, painful, involvement of mucosa, generalized rash
Stevens Johnsons Syndrome/Toxic Epidermal Necrolysis
This is rare, Incidence - 7 persons/million and almost always associated with a drug (77-95%). The other cause is usually Mycoplasma pneumonia. Unfortunately, it can range up to 45 days from drug or pna to disease process.
Drugs - Most common = Allopurinol
- Anti-gout
- Antibiotics (sulfa>pcn>cephalosporin)
- Antipsychotics
- NSAIDs
Pathophysiology
SJS/TEN is caused by kerotinocyte cell death from massive accelerated apoptosis via cytotoxic T cells
*Key Protein = Granulysin
- A cytolytic protein released from natural killer cells it is a mediator for kertoinocyte death
- Fluid levels of granulysin from blisters from SJS/TEN correlate with severity of disease
HLA reaction to T lymphocytes initiates the immune reactions of SJS/TEN
ie HLA-B*1502 strongly associated with carbamazepine induced SJS
Presentation
New medication leading to Rash
Patients start with viral appearing illness then develop the mucocutaneous lesions
SJS/TEN a spectra by severity
SJS less severe with sloughing < 10% BSA
TEN (Lyell’s Syndrome) is sloughing >30% of BSA, always involves mucous membranes
Rash
Lesions are symmetrically distributed, start on the face and thorax before spreading to other areas
Palms and soles are usually not involved. This is the opposite of tick borne rash.
Confluent erythema (erythroderma)
Conjunctival lesions (85%)
Facial edema
Palpable purpura
Skin necrosis with epidermal detachment +Nikolsky sign
Blisters and/or epidermal detachment
 Rash of Steven's - Johnson's
Rash of Steven's - Johnson'sLaboratory results
- Anemia
- Leukopenia
- Neutropenia (⅓) - correlated with poor prognosis
- Elevation in aminotransferase (2-3x normal) in 50%
Diagnosis - Just keep it on your differential and consider collecting blister fluid for Granulysin
- A suggestive history with drug exposure or illness (usually mycoplasma pna)
- A prodrome of acute onset illness/malaise
- Erythematous macules, targetoid lesions, or erythma progressing with vesicles and bullae
- Necrosis and sloughing of the epidermis
- Biopsy to exclude other disease
- Serum Granulysin from fluid from blisters
Mortality
- Higher mortality with comobid illness
- Retrospective study found 14/18 pts who died had HIV, DM, or Alcoholism
- Higher mortality with antimicrobials, Anti-epileptics, and NSAIDs
- Decreased mortality with M pneumonia induced SJS
Treatment
Supportive Care
There is a large amount of literature looking at both steroids and IVIG. No RCT exist for either due to low prevalence/high mortality. In general IVIG has more positive outcomes especially if given early in the disease process. Refer to your local emergency dermatologist.
References
- Chapman. Diagnosis and Management of TIckborne RIckettsial DIseases: Rocky Mounted Spotted Fever, Ehrlichiosis, and Anaplasmosis - United States. National Center for Infectious Diseases CDC.
______________________________________________________
Case Questions:
1. July you are practicing at a rural hospital in Missouri when a 5 year old girl presents with 3 day history of intermittent fevers, headache, nausea and sore throat. Vitals include fever 103F, and she has a maculopapular rash on her legs, including the soles of her feet. What is the appropriate work-up?
1. July you are practicing at a rural hospital in Missouri when a 5 year old girl presents with 3 day history of intermittent fevers, headache, nausea and sore throat. Vitals include fever 103F, and she has a maculopapular rash on her legs, including the soles of her feet. What is the appropriate work-up?
a. CBC, chemistry, rapid strep, IgG, IgM for Rickettsii, consider spinal tap, broad spectrum antibiotics with doxycycline
b. Discharge with alternating tylenol/motrin every 4 hours and follow-up with primary care doctor
c.CBC, chemistry, CT scan, LP, neuro consultation, central line, broad spectrum antibiotics, ICU admission
d. Treat with zofran and 20mg/kg fluid bolus and reassess
2. What is the appropriate treatment for the above illness?
a. Vancomycin/Zosyn
b. No antibiotics needed, family reassurance and primary care follow-up
c. Admission with supportive care
d. Doxycycline
3. What is the appearance of the rash for Rocky Mountain Spotted Fever?
a. Large red slowly spreading rash with central clearing
b. Rash usually 2-5 days after fever, initially small pink macules on wrists/ankles including palms/soles later petechia
c. Mucous membrane involvement with lesions symmetrically distributed, start on the face and thorax before spreading to other areas
d. Acute exfoliation of the skin followed by an erythematous cellulitis
4. 56 year old woman with a history of recent UTI presents with a rash. Patient states she was on bactrim for a pyelonephritis for the past 2 weeks and developed a rash 3 days prior. Patient is ill appearing with lesions on the face and thorax involving mucous membranes. Palms and soles are not involved. Lesions initially were red with dark centers but now are dusky with central bulla. Patient is hypotensive. What is the appropriate work-up?
a. CBC, chemistry, blood and urine cultures, institute early goal directed therapy, fluids and possibly pressors.
b. CBC, chemistry, blood and urine cultures, fluid resuscitation, nutritional supplementation, wound care. Consult dermatology and consider transfer to burn center.
c. CBC, chemistry, rapid strep, tick panel, consider spinal tap, broad spectrum antibiotics with doxycycline
d. CBC, chemistry, CT/LP, fluid resuscitation
ANSWERS BELOW
1. a
2. d
3. b
4. b
No comments:
Post a Comment