

Case Introduction:
A 25 year old female presents to your emergency department
after a bicycle accident one day prior.
Yesterday afternoon, she had been training for the “FAT TIRE” mountain
bike race when her front tire lodged between a rock crevice on a downhill path. She cannot recall all of the details but
knows that she stopped abruptly, launched forward hitting her handlebars, then
separating from her bike. She denies
hitting her head or loosing consciousness but notes that she landed on her
right shoulder and “it hurts.”
She awoke this morning with notable left upper abdominal pain
and a sensation of “fullness” in her belly.
Upon standing she developed lightheadedness and passed out landing face
forward on the bedroom floor and sustaining a cut to her nasal ridge.
In the emergency she reports ongoing abdominal pain and R
shoulder pain. No nausea or vomiting. She is not on anticoagulants.
Initial Vital Signs:
Temp: 97.0 °F (36.0
°C) BP: 85/53 mmHg Pulse:
95 Resp: 17 SpO2: 99 %
Physical Exam:
Primary Survey:
Airway: Patent, phonating normally
Breathing: Normal chest rise, bilateral breath sounds present
Circulation: Warm to touch, pulses intact, hypotensive
Secondary Survey:
General: Awake, alert, severe distress
HEENT: Abrasion over
the nasal ridge, bleeding controlled, EOMI, PERRL.
Neck: Tenderness to
palpation over C6
Cardiac: regular rate and rhythm, no murmur/rubs/gallops
Respiratory: Clear to auscultation bilateral
Abdomen: Tenderness
to palpation diffusely with guarding, peritoneal signs present
MS: tenderness over
the L elbow, bruising over L arm,
Neuro: Cranial nerves 2-12 intact, normal sensation
throughout
Extremities: No lower extremity edema, distal pulses intact
Psychiatry: Appropriate

Take a brief Cognitive Pause….What worries you about this
case?
- ABNORMAL VITAL SIGN (BP 85/53)
- “Separated from bike”
- Peritoneal signs on abdominal exam
- “passed out”
- C6 tenderness
Enough with the cognitive moment…Time for ACTION!!!

- gain vascular access with 2 large bore IV’s and initiate NS
bolus

- place c-collar for neck stabelization

- perform bedside FAST which shows free fluid in morrison’s and splenorenal pouch

- page Level 1 trauma requesting immediate surgical evaluation in the ED


- call for uncrossed O negative blood, ie. The Massive Transfusion Protocol

The case continues; and patient responds to IV normal saline. Her pressure improves to 101/65. She has portable chest and pelvis xrays which are unremarkable.
Fentanyl is given for analgesia.
Surgery evaluates the patient in the Emergency Department and
recommends urgent transfer to Level I trauma center.
She is rapidly transferred by EMS to a nearby Level I Trauma
Center.
Her vital signs remain stable and she undergoes a “PAN SCAN”
(Head, Neck, Chest, Abdomen, and Pelvis.)
The CT scan shows a high grade splenic laceration with a “contrast
blush” within the splenic parenchyma.
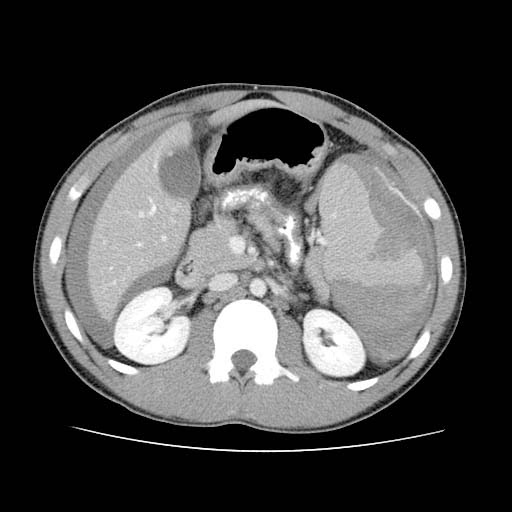
Hemoperitoneum (thick grey outline surrounding both liver and spleen)

Contrast Blush (blue arrow)

For more information about splenic injuries and radiology, check out this cool site: Learning Radiology
_______________________________________________________________
Case Discussion:
(Much of this discussion was modified from the October 2013 North Memorial Trauma Update)
I think the
hardest thing about Abdominal Trauma (for us and our patient population) is
remembering to consider abdominal trauma when it may not be obvious, or when
there are other distracting injuries present. Motor vehicle and bike accidents are obviously concerning mechanisms, but what about the elderly patient with dementia who suffers an unwitnessed fall?
Blunt
liver and spleen injuries are very common and occur from a variety of
mechanisms. In fact, in blunt trauma, the
Often, the
physical exam for diagnosis of intra-abdominal blunt injuries is woefully
inaccurate. Factor in abnormal mental status exam, dementia, drugs, or
chemicals, and the accuracy of physical exam gets even worse. In this case, it was apparent that the patient
had abdominal pain and needed full trauma evaluation. Unfortunately it isn't always this easy.
If you suspect a spleen or
liver injury in a patient who has suffered trauma, whether because of
concerning mechanism or abdominal tenderness on exam, you need to first assess hemodynamic
stability.
If the patient is hemodynamically UNSTABLE (meaning they have low blood pressure and DO NOT respond to IV fluids)…they need a surgeon and an operating room NOW. If you suspect abdominal trauma you should always perform a bedside FAST exam
to assess if there is free-fluid in the belly.
Bedside ultrasound remains a popular and widely-used method of assessment in the ED. It's sensitivity for blood in the abdomen (hemoperitoneum) varies from 60-99% depending on the operator. It is not perfect, but if you see fluid you've a just given yourself and more importantly the patient a jump start to definitive care. "USE-IT" !!!
If the patient is
hemodynamically STABLE, you may want to consider getting a CT with IV
contrast.
IV contrast-enhanced CT scan of the abdomen is the diagnostic procedure of choice for diagnosing intra-abdominal trauma.
Accuracy approaches 98% in blunt liver and spleen trauma. This is also an excellent way to find other
associated intra-abdominal injuries.
There is a
standardized injury severity grading system determined from CT images done with
intravenous contrast. If you'd like to know more about this check out the link: Injury Scale
The most
common types of blunt liver and spleen injuries include subcapsular hematomas
and lacerations. These are
usually managed non-operatively. In fact, it is now standard
for 90% of splenic injuries are to be managed Non-operatively. NOM
has become standard practice with studies showing shorter
hospital lengths-of-stay, lower hospital costs, decreased infection rates, and
even decreased morbidity and mortality.
Can we predict who is the best candidate for non-operative managment?
Two
radiologic features that are searched for on the initial abdominal CT scan are
the presence of active hemorrhage
(extravasation) or an intraparenchymal
vascular injury referred to as a “contrast
blush.” (Both are seen in the images above.)
Active
hemorrhage often results in a patient becoming hemodynamically unstable, and usually requires urgent operative intervention.
Contrast
blush can be found in a hemodynamically-stable patient and may
represent either a traumatic pseudoaneurysm or a traumatic arteriovenous
fistula. The presence of blush predicts a higher risk of
re-bleeding (20 times the risk of re-bleed) and in turn a higher likelihood that non-operative management will fail.
One of the reasons for the increased success of non-operative management has been the advancement of angiography and embolization. Basically, the interventional radiologist enters into the femoral vein with a catheter and attempts to "plug" (unofficial term) the bleeding vessels using a "coil".

Interestingly, as of yet there are no
widely-accepted indications for the use of angiography and embolization; because there are no significant studies. However, as it stands, the presence of a vascular blush in a
hemodynamically stable
patient with blunt splenic injury, should lead to strong consideration of early
angiography.
______________________________
Case conclusion:
Our patient undergoes angiography and embolization is attempted. She unfortunately re-bleeds and ultimately requires open laparotomy and splenectomy.
She recovers well and continues to mountain bike regularly.
The end.

Case Questions:
1.
FAST
stands for:
a.
Formal
Assessment and Surgical Technique
b.
Focused
Assessment with Sonography for Trauma
c.
Frenetic
Accusation of Someone named Tom
d.
Forceful
Aspiration of Sonographic Tissue
2.
The
sensitivity of FAST for blood in the abdomen ranges from 60-99% depending on:
a.
The
operator
b.
The
patient
c.
The
time of day
d.
The
day of the week
3.
If
a patient is hemodynamically unstable (and does not improve with IV fluids) you
should immediately:
a.
Send
the patient to the CT scanner
b.
Perform
an open laparotomy in the Emergency Department
c.
Transfer
the patient to a Level I trauma center for immediate surgical intervention
d.
Page
the on-call surgeon and wait and wait indefinitely for a return call
4.
If
a patient is hemodynamically stable they are likely a candidate for:
a.
Non-operative
Management
b.
Elective
splenectomy
c.
Tummy tuck and breast augmentation
d.
The
2016 presidential race
5.
True or False: There are widely accepted
indications for the use of angiography and embolization in cases of splenic
injury.
a.
True
b.
False

1. b
2. a
3. c
4. a
5. b
Thanks for playing!
No comments:
Post a Comment