
Pediatric Case of the Week #2:
A 4 year old boy is brought to your Emergency Department with the Chief Complaint of: Limp

His parents note that he has had a limp for the past 5 days. It seemed to occur after he tripped while playing and has become progressively worse. He can no longer bear weight on his left leg.
His parents also report that he has had a low grade fever over the past 2 days. He was treated for otitis media 2 weeks ago and has subsequently finished a course of augmentin.
VS: T 101.8 BP 115/68 Pulse 108 RR 22
What is your next step?
What is the most likely diagnosis (or list of diagnoses)?
_____________________________________
Wednesday Update:


__________________________________________________________________________
Friday Update:
Final thoughts (gleaned from Pediatric Textbook of Emergency Medicine, and August EM RAP lecture by Ilene Caudius):
Most kids with septic hip look sick. A child with septic hip will often maintain a position of comfort which is most often flexed at hip and externally rotated (the opening picture above is therefore misleading.)
Clinical exam matters in making the diagnosis of septic hip. Most kids with septic hip will resist even the slightest joint motion. Dr Claudius recommends treating with an NSAID then sending the child to xray. If you can range the joint or the child will bear weight after returning from xray, she would avoid Ultrasound. She notes that this is because 50-90% of Transient Synovitis will have an effusion...and once you find an effusion you are COMMITTED TO TAPPING THE JOINT.
This is different from my training. I was taught to ultrasound liberally, if an effusion is present, the joint should be tapped. Unfortunately, there is no 'fool proof' algorithm. Physician clinical judgement, patient/family risk tolerance, and physician risk tolerance are all factors in determining best practice.
Dr Claudius would not recommend starting antibiotics prior to tapping the joint. (In cases where I would be transferring a child to Children's for joint tap, I personally would want to start prophylactic antibiotics.) I would specifically discuss the question of prophylactic antibiotic administration with the Children's PEDIATRIC EM attending prior to transfer and document his or her recommendations.
Final Final Thoughts: (Gleaned from; Avoiding Common Errors in the Emergency Department)
1. Always consider fracture and get an Xray
2. Always consider non-accidental trauma (Child Abuse)
3. Osteomyelitis and Septic joint should be high on differential list and treatment should be prompt.
4. Consider OTHER potentially lethal diagnosis; malignancy, abdominal infection. All that limps is not musculoskeletal.
A 4 year old boy is brought to your Emergency Department with the Chief Complaint of: Limp

His parents note that he has had a limp for the past 5 days. It seemed to occur after he tripped while playing and has become progressively worse. He can no longer bear weight on his left leg.
His parents also report that he has had a low grade fever over the past 2 days. He was treated for otitis media 2 weeks ago and has subsequently finished a course of augmentin.
VS: T 101.8 BP 115/68 Pulse 108 RR 22
What is your next step?
What is the most likely diagnosis (or list of diagnoses)?
_____________________________________
Wednesday Update:
With a little training, you could perform a bedside Ultrasound:
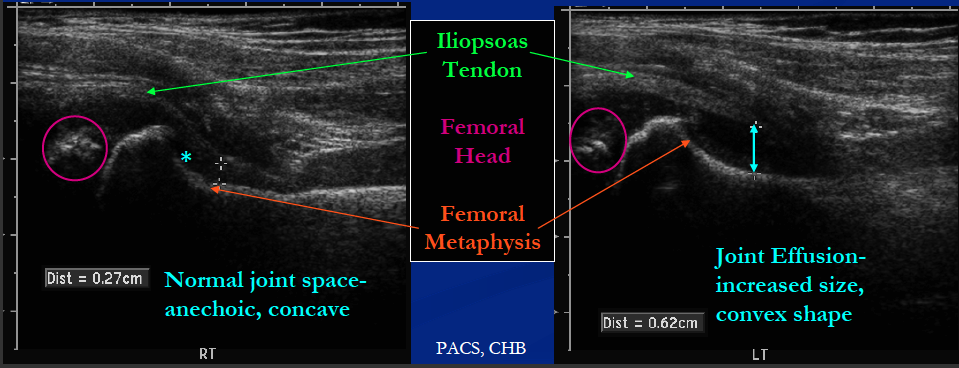
See this Video regarding adult hip ultrasound: http://www.youtube.com/watch?v=0Fu4R9mEoz4
See this ACEP link regarding pediatric hip ultrasound: http://www.acep.org/Education/Continuing-Medical-Education-(CME)/Focus-On/Focus-On--Pediatric-Hip-Ultrasound/
See this ACEP link regarding pediatric hip ultrasound: http://www.acep.org/Education/Continuing-Medical-Education-(CME)/Focus-On/Focus-On--Pediatric-Hip-Ultrasound/
__________________________________________________________________________
Friday Update:
Final thoughts (gleaned from Pediatric Textbook of Emergency Medicine, and August EM RAP lecture by Ilene Caudius):
Most kids with septic hip look sick. A child with septic hip will often maintain a position of comfort which is most often flexed at hip and externally rotated (the opening picture above is therefore misleading.)
Clinical exam matters in making the diagnosis of septic hip. Most kids with septic hip will resist even the slightest joint motion. Dr Claudius recommends treating with an NSAID then sending the child to xray. If you can range the joint or the child will bear weight after returning from xray, she would avoid Ultrasound. She notes that this is because 50-90% of Transient Synovitis will have an effusion...and once you find an effusion you are COMMITTED TO TAPPING THE JOINT.
This is different from my training. I was taught to ultrasound liberally, if an effusion is present, the joint should be tapped. Unfortunately, there is no 'fool proof' algorithm. Physician clinical judgement, patient/family risk tolerance, and physician risk tolerance are all factors in determining best practice.
Dr Claudius would not recommend starting antibiotics prior to tapping the joint. (In cases where I would be transferring a child to Children's for joint tap, I personally would want to start prophylactic antibiotics.) I would specifically discuss the question of prophylactic antibiotic administration with the Children's PEDIATRIC EM attending prior to transfer and document his or her recommendations.
Final Final Thoughts: (Gleaned from; Avoiding Common Errors in the Emergency Department)
1. Always consider fracture and get an Xray
2. Always consider non-accidental trauma (Child Abuse)
3. Osteomyelitis and Septic joint should be high on differential list and treatment should be prompt.
4. Consider OTHER potentially lethal diagnosis; malignancy, abdominal infection. All that limps is not musculoskeletal.
Dr. Tom,
ReplyDeleteWhat is the window being used to get this view?
Great question!!!
DeleteFor adult you would use the curvilinear probe (abdominal probe) but for the pediatric patient, with less superficial tissue, you would use the high-frequency (5-10MHz) linear transducer. I will include two references (links to augment this discussion.)